



|
.png)
|
|
|

|
Search
05/18/2023
RESPONSES/COMMENTS
RE: Unequal Treatment of Ex-Patriot DPMs by ABPM
From: Jeff Carnett, DPM
There are many of us American trained DPMs working overseas who are not eligible to be board certified by either board as we did one or two-year residencies, but not three-year programs. So, how shocking to see that ABPM will certify those with bachelor degrees in podiatry from the UK, SA, Australia, Malta, and New Zealand who did not take the MCAT, have no basic medical sciences in their courses, and no residencies. These degrees are right from high school.
Doesn't that discredit anyone with the ABPM certification in the U.S.? So, we expatriate DPMs need to take a bachelor podiatry degree so we can get certified, but we can't get certified with a CPME-approved DPM degree and residency? I’m trying to understand how that helps the profession. While overseas, our work is often highly surgical, but alas that doesn't count.
Jeff Carnett, DPM. Auckland, New Zealand
Other messages in this thread:
08/01/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1D
RE: The Passing of Arthur Ervin Helfand, DPM
I am deeply saddened hearing the news of the passing of Arthur Helfand He was both a mentor and friend over many years. He brought our profession to a higher standard in the medical community in the 1960s and 70s. He was instrumental in guiding and encouraging me to apply to the Johns Hopkins School of Public Health. I was the first podiatrist who was accepted for an MPH degree when only medical doctors, dentists, and nurses were accepted there.
He gave me the opportunity to open up our profession to a higher standard of acceptance throughout the medical community. An MPH degree for podiatrists is now encouraged and sought after by many graduates, becoming of part of the mainstream healthcare community.
My heartfelt condolences to his family and friends.
Joseph S Fox, DPM, MPH
08/01/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1C
RE: The Passing of Arthur Ervin Helfand, DPM
The profession lost one of its greats. Unfortunately, many of the younger podiatrists likely never knew him or even heard of him. Dr. Helfand was also my teacher. I still remember his “hey Doc” salutations, his slight smile, his love of teaching. He was one of our professions’ leaders. He was critical part of the St Luke's Residency in Philadelphia. He one of the first podiatrist to enter the hallowed halls of allopathic medicine in Philadelphia. Truly a pioneer. He was one of the luminaries of our profession. He was always around others bigger than life podiatrists such as Dr. Irv Kanat.
One personal story. When I graduated Temple, my first job was at the VA in Washington, DC. Out of the blue comes a letter from Dr. Helfand. He said the APMA attorney had a beautiful daughter and I should call her. We’ll that letter went in my wallet. Several months later, I was cleaning out my wallet and found that letter which I thought I threw away. I was never a big fan of blind dates but decided what the heck!. Well, now 46 years later, that girl still has the same twinkle in her eyes, with plenty of kids and grandkids, all the result of Dr. Helfand. I still have that note.
Lawrence Oloff, DPM, San Francisco, CA
08/01/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1B
RE: The Passing of Arthur Ervin Helfand, DPM
Very simply, Arthur Helfand was a mensch! May his memory be for blessings.
Arden Smith, DPM
Arthur Helfand DPM, was a legend long before there was such a field called podiatric medicine and surgery. Art was a chiropodist by training and if it wasn’t for Arthur, I would never had applied to the Giuffre College of Podiatry at St. Luke’s Hospital. I was in the First class of what became the Pennsylvania College of Podiatric Medicine. He along with Jim Bates, DSC assured me that we would graduate as podiatrist, and a new day was arising from the ashes of Temple University College of Chiropody.
Art was smart, a graduate of Central High in Philly, that had more Mensa people come out of that high school than most. He was a passionate, caring human being. Always pushing students to do better. Through his close relationship with...
Editor's note: Dr. Sokoloff's extended-length letter can be read here.
08/01/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1
I was saddened to see the article announcing the passing of Dr. Helfand. From June 1975 until May 1976 Dr. Helfand was my director of residency at St. Luke’s and Children’s Hospital Philadelphia. He gave all his residence great advice and was always ready to listen to the newest podiatrists to our profession.
Joseph Sidone, DPM
I was saddened to learn of Arthur's passing. I worked with him at PCPM for many years; he was a tireless champion of Podiatric Public Health and a very prolific health care writer for the profession while at PCPM. He was the consummate gentleman. He served the profession with rare enthusiasm, hard work, and honor. RIP Arthur.
Harold W. Vogler, DPM
07/31/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 2B
I am saddened by the loss of Biff Kramer. He was a major force in the APMA. We served many years together at the APMA House of Delegates. Together we formed the Mid-States Coalition to facilitate elections and passage of key Resolutions. We have lost another pioneer.
Joel A. Feder, DPM
07/31/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 2A
RE: The Passing of Bruce "Biff" N. Kramer, DPM
Biff Kramer was so many things to so many people in more ways than most - a mentor to some and a hero to others. He was a major part of so many communities, including our own. For me, Biff was a mentor in the world of APMA politics. I got to know Biff during my early years at the HOD where I spent (what seemed like) hours standing at the back of the House with him. I always looked forward to his advice, counsel, and friendship over the years. My condolences to Heather and family as well as all of Biff's extended families within the communities he built.
Marlene Reid, DPM
07/31/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1D
RE: The Passing of Arthur Erwin Helfand, DPM
“Illustrious career” does not begin to capture the totality of contributions Dr. Helfand made to advance our profession. As students at PCPM in 1972, we all were aware that Dr. Helfand was passionate about public health and geriatric medicine. I remember so well how, in 1972, he told our class that the future of podiatry would be in diabetes and geriatrics. This was in 1972! I remember thinking how ridiculous this was. Diabetes? Geriatrics? What was this guy thinking about? Well, here we are in 2026. And he was correct, as he always was. He was highly respected in the general medical professions as he was in podiatry. He was an inspirational teacher, a scientist, an effective leader. Our inclusion in Medicare, the ability to prescribe physical therapy, the development of residency education, were to a large extent the result of his work and the respect for his accomplishments by those outside of podiatry.
If there were a Mount Rushmore of podiatry, his likeness would be gracing the entity. He was a powerful, pragmatic, humble but effective force which in no small way advanced our profession to its current state. Thank you for all you had the foresight to have done for podiatry Dr. Helfand. Those of us old enough understand and are forever grateful for your devotion and accomplishments for all of us.
Allen M. Jacobs, DPM
07/31/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1C
RE: The Passing of Arthur Erwin Helfand, DPM
I write with a heavy heart to mark the passing of Dr. Arthur Helfand. I first encountered him in 1984 as a student at the Pennsylvania College of Podiatric Medicine, and again from 1988 to 1989 as a resident (in my first residency) under his direction at the James C. Giuffre Medical Center — the oldest podiatric residency program in the country. As class president in 1987, I dealt with Arthur directly and often. One thing was never in question: he held the student and the educational process above all else, often above the interests of other faculty. That priority shaped how he led.
Arthur and I did not always agree. In fact, we found ourselves on opposite sides of more debates than I can count, including years later when I served as president of what is now the American College of Podiatric Medicine. But disagreement with Arthur was never petty — he argued from conviction, from decades of study, and from a genuine love of this profession. I always respected where he stood, even when I stood elsewhere.
His record speaks for itself: a past president of our national association, a champion of geriatric care for over sixty years, and for much of his career a quiet hand guiding many of our profession’s leaders from behind the scenes. He was a well-educated, deeply engaged contributor — a true harbinger of where podiatry needed to go.
Bret Ribotsky, DPM, Fort Lauderdale, FL
07/31/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1B
RE: The Passing of Arthur Erwin Helfand, DPM
I am totally saddened by this bad news. So many of us worked with Dr. Helfand in so many different capacities. As president of the American Society of Podiatric Medicine, which was the oldest subspecialty group affiliated with the APMA, Dr. Helfand was active on our board of directors. He attended every meeting and helped guide us in every aspect of our existence. Of course, his pet projects dealt with podiatry and aging, and Dr. Helfand strongly expressed the fact that dentistry and so many other branches of healthcare have societies dedicated to the aging patient. To this end, we sponsored and gave lectures at various podiatric conferences on podiatry and aging.
In memory of Dr. Helfand we will devote our resources in the American Society of Podiatric Medicine to foot care and the aging patient. My last conversation with him was exactly on this. I invite anyone interested to contact me directly so that we can fulfill what meant so much to Dr. Helfand and may his memory be a blessing for all of us.
Elliot Udell, DPM
07/31/2026
RESPONSES/COMMENTS (OBITUARIES) - PART 1A
RE: The Passing of Arthur Erwin Helfand, DPM
Dear friend, mentor, and colleague, I learned so very much from you over the years and will greatly miss your advice and counsel. Thank you. Rest in Peace.
David George, DPM
I count myself fortunate to have been among the scores of podiatrists who trained under Art Helfand. He was a podiatrist for all podiatrists. Whether it was teaching, lecturing, writing and publishing, or holding various leadership offices within the profession, Art was always available to chat and inspire. He was a straight shooter and his advice was always welcome and spot on. Without a doubt, he was a giant in our profession. My deepest condolences to Myra, Louis, and Jennifer.
Jeffrey S. Gerland, DPM
07/29/2026
RESPONSES/COMMENTS (CLINICAL)
RE: Prehabilitation for Patients Undergoing Elective Foot and Ankle Surgery
From: Paul Kesselman, DPM
This recent article came across my desk as a peer reviewer for insurance companies. This article is no doubt an interesting read for those with active operating privileges, or even for those non-surgical physicians who may ultimately refer a patient to a colleague for foot/ankle surgery. I am wondering what others may think.
Paul Kesselman, DPM, Oceanside, NY
07/28/2026
RESPONSES/COMMENTS (STUDENT RECRUITMENT)
RE: Motivations, sources of influence and barriers to being a podiatrist: a national questionnaire of student views
From: Allen Jacobs, DPM
This study is an interesting analogy to our current student recruitment process.
Allen Jacobs, DPM, St. Louis, MO
07/28/2026
RESPONSES/COMMENTS (PODIATRIC ECONOMICS)
RE: Little Financial Incentive to do Surgery
From: Gregory Eirich, DPM
It is hard to justify the financial incentive to do surgery. With a 90-day global fee for follow-up, there are procedures that we will lose money throughout the peri-operative period. When I started practice in 1991, the Anthem reimbursement for a chevron-type bunionectomy was just over $1,200 ($2,942 in 2026 dollars). Today, I get just under $600.
This means making less than one quarter the money with the same liability, What is the sense in doing surgery?
Gregory Eirich, DPM, Tustin, CA
07/27/2026
RESPONSES/COMMENTS (MEDICAL TEACHING)
RE: Medical Teaching
From: Rod Tomczak, DPM, MD, EdD
Over the last several months we have beat podiatric education, the schools, students, degrees, admissions, APMA, CPME, and AACPM to death. We have neglected to discuss the faculty, teaching, and the question of who makes up the schools, students, or faculty.
I have heard the pseudo-podiatry professors boast of their classroom acumen based on the fact they have given a lecture on hammertoes to their local podiatry academy and wrongfully belittle podiatry school faculty with the age-old adage that those who can do and those who can’t teach. Teaching at a podiatry school is not seeking refuge and a ride on the gravy train. When invited to the colleges to guest lecture they politely refuse, but some come and a few experience their first panic attack in front of a classroom of students better read than...
Editor's note: Dr. Tomczak's extended-length letter appears here.
07/24/2026
RESPONSES/COMMENTS (PODIATRIC ECONOMICS)
From: Ivar E. Roth, DPM, MPH
Dr. Freireich has brought up some great points. I think the APMA needs to set up a committee to discuss what to do. The hospitals are hiring away all the private practice doctors and of course enjoying the income from the ancillary services they offer. We as a profession need to have a seat at the table or come up with a strong solution before private practice really dies. Any ideas?
Ivar E. Roth, DPM, MPH, Newport Beach, CA
07/24/2026
RESPONSES/COMMENTS (PM NEWS QUICK POLLS)
From: Elliot Udell, DPM
In the current survey on PM News, only 6% of the responders indicated that they give out brochures to pre-med students on careers in podiatry. Perhaps some of these doctors can inform the rest of us where to obtain these handouts. Does the APMA or state societies furnish these? Yesterday, I had a 3rd year college student in my office. I was telling him all about podiatry as a career but would have loved to be able to hand him a professionally-made brochure.
For months, we have been debating the possible reasons why our schools may not be filling their classes. Handing out brochures in all of our offices might be a simple fix.
Elliot Udell, DPM, Hicksville, NY
07/23/2026
RESPONSES/COMMENTS (PODIATRIC ECONOMICS)
from: Ron Freireich, DPM
I'm going to offer a much more simple answer to this question...surgical fees have decreased because we collectively as a profession allowed it to happen. As Dr. Jacobs stated, a 49% decrease in surgical fees over the last 25 years. I have another question, when is enough going to be enough? It wasn't enough when surgical fees decreased 15%, 25%, or even 40%. And now at 49%; will this be enough? I don't think so because there is absolutely no pushback from anyone and there never has been. What an embarrassment for this profession. I can't think of any other profession that has allowed this to happen to themselves.
So let me get this straight: a podiatry student who attends podiatry school for four years after investing around three hundred thousand dollars and completes a three-year surgical residency will be able to use their highly trained knowledge, surgical skills, and experience to generate ancillary income for the hospital by ordering radiology, PT, DME, etc. to supplement their salary, instead of being reimbursed a reasonable fee for their surgical procedures.
In other words, a high value is placed on the simplicity of placing orders and a low value is placed on the complexity of doing surgery. Shouldn't podiatric surgeons be reimbursed a reasonable fee in addition to generating ancillary income for the hospital? The ancillary fees that a surgeon generates, in my opinion, won't be sustainable in the future. A 49% decrease in reimbursements in the last 25 years... does anyone really think the insurance companies are going to stop the cuts now?
Ron Freireich, DPM Cleveland, OH
07/23/2026
RESPONSES/COMMENTS (CLINICAL)
From: Ivar E. Roth, DPM, MPH
I can speak directly to the MIS bunionectomy. I am currently using the MiniLock system, and I am very happy with the results, especially with the sesamoid positioning post-correction. While it is technically challenging for someone trained in open surgery, it does not have a steep learning curve.
Concerning the splint issue, please provide a link so we can see for ourselves about the claim issues being made. From my perspective, any DPM who claims a splint can fix a bunion is a snake oil salesperson and should be investigated for their false claims. Can anyone opine on who would investigate and or take action concerning false claims within our profession.
Ivar E. Roth, DPM, MPH, Newport Beach, CA
07/23/2026
RESPONSES/COMMENTS (AI)
From: Patrick DeHeer, DPM
I want to echo Dr. DeSantis' comments regarding the potential of ambient AI documentation. While individual physicians will ultimately determine which platform best fits their practice, there is little question that artificial intelligence is rapidly becoming an important tool for improving efficiency, reducing administrative burden, and allowing physicians to spend more time focused on what matters most: caring for patients.
As our profession embraces these technologies, I also share Dr. DeSantis' hope that companies choosing to invest in podiatric medicine will become true partners in advancing the profession. One of the most meaningful ways they can do that is by supporting the APMA Educational Foundation through scholarships, educational programming, and initiatives that help reduce financial barriers for students pursuing careers in podiatric medicine.
Our students represent the future of the profession. Investing in their education is an investment in better patient care, stronger advocacy, and the continued advancement of podiatric medicine. I encourage industry partners who recognize the value of our specialty to consider supporting these efforts and helping us develop the next generation of podiatric physicians.
Patrick DeHeer, DPM, Indianapolis, IN
07/22/2026
RESPONSES/COMMENTS (CLINICAL)
RE: New Bunion Splints vs. New MIS Bunion Procedures
From: Evan F. Meltzer, DPM
Lately, I have been seeing posts on Facebook about a new bunion splint. The first few posts were clearly advertising the splint as a permanent solution to correct a painful bunion deformity without surgery. The last post I read was another advertisement for the splint, but this one was endorsed by one of our podiatric colleagues. She incorrectly emphasized the exaggerated costs of the surgery, the extensive recovery time, and recurrence rate following surgery. Of course, we all know that she is being compensated for her endorsement of this splint.
I retired before the introduction of the new MIS bunion procedures, but having done many successful bunion surgeries in the traditional method, it seems that the newer MIS procedures might have faster recovery times and less visible incisions. If this new splint “cures” bunions, then the biomechanics I learned at PCPM in the '70s and my own experience of 40+ years of practice must not have counted with respect to bunion surgery. I would appreciate hearing from my colleagues about their experiences with the new MIS procedures for bunions and their thoughts about this new “miracle” splint.
Evan F. Meltzer, DPM (retired) Rio Rancho, NM
07/21/2026
RESPONSES/COMMENTS (THE FUTURE OF PODIATRY)
RE: AI’s Take on Podiatry’s Future
From: Lawrence Rubin, DPM
I asked AI to comment on whether today's podiatry residents would be better served by fellowships in lower extremity medicine rather than advanced surgery. AI's response was thought-provoking:
"Rather than replacing advanced surgical fellowships, podiatry should consider adding accredited fellowships in Lower Extremity Medicine. As healthcare shifts toward value-based care, prevention, chronic disease management, diabetic limb preservation, peripheral neuropathy, PAD, wound care, and multidisciplinary leadership are becoming increasingly important. Complex reconstructive surgery will always be essential, but far more patients need expert medical management than advanced surgical reconstruction. Parallel fellowship pathways—one in advanced surgery and one in comprehensive lower extremity medicine—could better prepare future podiatrists for tomorrow's healthcare environment."
Lawrence Rubin, DPM, Las Vegas, NV
07/21/2026
RESPONSES/COMMENTS (PM NEWS QUICK POLLS)
From: Chris Robertozzi, DPM
The results reinforce what I heard from a newly accepted student. In order to complete their acceptance, candidates must get a letter of recommendation from a podiatrist. The student emailed me to see if she could visit my office and if I would write a letter of recommendation for her. I was happy to have her visit the office. She asked me if I enjoyed what I did every day. I responded, of course, I love it. She told me that I'm the only podiatrist that she visited who was happy with their career. With only 7% of the profession having brochures in the office about the profession and not only being unhappy with our profession but telling others that, maybe we are part of the recruitment problem.
My guess is that those who are unhappy with the profession are really unhappy with the way we are treated by the insurance companies and not the care that we provide. I'm not happy with the way all of health is treated by the insurance industry, but I am happy working with patients and being able to make a difference in their lives and keeping them walking.
Chris Robertozzi, DPM, Newton, NJ
07/20/2026
RESPONSES/COMMENTS (PODIATRIC STUDENT ENROLLMENT)
From: Alan Sherman, DPM
Also demonstrated in the statistics from Wayne State Medical School is how competitive it was this year. They interviewed 11% of their applicants and matriculated 2%. This seems to be a microcosm and not illustrative of all medical schools.
My favorite AI is telling me that this year, 35% to 45% of applicants to MD and DO schools were matriculated. It makes you wonder why Wayne State was so much more selective? The year I applied in 1977, medical schools across the board accepted 11% of applicants.
Alan Sherman, DPM, Boca Raton, FL
07/17/2026
RESPONSES/COMMENTS (PODIATRIC STUDENT ENROLLMENT)
RE: Podiatry's Student Enrollment Crisis
From: Seymoure Balaj,DPM
These statistics are from local Wayne State Medical School - Just one school. Look at the numbers!
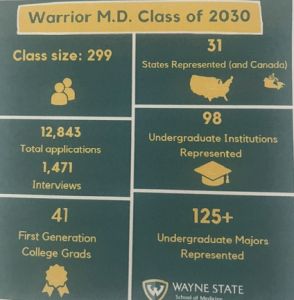 |
Wane State Medical School Class of 2030 |
This represents more applications to one medical college than all 11 podiatry schools combined! It tells you where the interest is and where the best go.
Seymoure Balaj, DPM, Southfield, MI
07/17/2026
RESPONSES/COMMENTS (DME)
From: Paul Kesselman, DPM
Let me say from the outset, that no one should ever be dissuaded from contacting their Congressional delegation about what they perceive as an unfair practice by CMS or any other Federal agency. That being said, the times are much different now than they were prior to the President’s State of The Union Address this past winter. Also Dr. Smith and Name Withheld DO NOT have the same scenario!
Having spent almost a decade on the DME Medicare Council, meeting with the NPE program directors, I am happy to provide some insight into their thinking and what is going on at CMS. I too have also been a victim of having my Medicare number stolen and having had numerous DME billed under my MCR number, which I both never received and never needed. So I support the Federal Government’s initiative to combat DME...
Editor's note: Dr. Kesselman's extended-length letter appears here.
|
| |

|
|
|

