|

|
|
|

|
PMNews
Browse PMNews Issues
Previous Issue | Next Issue
| PM News | |
The Voice of Podiatrists
Serving Over 12,000 Podiatrists Daily
March 13, 2010 #3,803  Publisher-Barry Block, DPM, JD Publisher-Barry Block, DPM, JD
A service of Podiatry Management http://www.podiatrym.com
E-mail us by hitting the reply key.
COPYRIGHT 2010- No part of PM News can be reproduced without the
express written permission of Kane Communications, Inc.
|
|
| PODIATRISTS IN THE NEWS | |
She's a Tri-athlete - Thanks to Total Ankle Replacement by WI Podiatrist
Roxanne Smothers wasn't physically active for 28 years until she had her left foot rebuilt and received her new "bionic" ankle. Since her total ankle replacement surgery in 2009, the 50-year-old Galesville woman has completed a triathlon and a 2,500-mile motorcycle trek. "I couldn't do anything," she said. In 1981, her foot and ankle were essentially crushed when a car struck her on a motorcycle, throwing her to the pavement. Doctors wanted to amputate her foot, but she and her family wouldn't let them. "Something had to be done. I was ready to have my foot amputated."
 |
| Dr. David Caldarella |
Smothers was referred to Dr. David Caldarella, a Gundersen Lutheran podiatrist who specializes in complex foot and ankle disorders, and reconstructive foot and ankle surgery. Caldarella first suggested a repositionable triple arthrodesis, which essentially straightened her overall foot alignment before the ankle implant.
Smothers had the foot surgery in December 2007 at Gundersen Lutheran. "Dr. Caldarella basically took my foot apart and put it back together with screws," she said. Total ankle replacement implants have been around for decades, but failed miserably with lots of complications in the 1960s and 1970s, Caldarella said. "With improvements in technology, engineering and knowledge of biomechanics, the implants are now excellent," Caldarella said. "But still it's never an ideal solution to replace the ankle, and surgery is the last resort." Total ankle replacement offers hope for chronic sufferers of ankle arthritis, Caldarella said.
Source: Terry Rindfleisch, Winona Daily News [3/10/10]
|
|
| PODIATRISTS IN THE COMMUNITY | |
AZ Podiatrist Donates Diabetic Shoes to Mission
About 200 people with diabetes will receive a new pair of diabetic shoes for free, thanks to a donation from Yuma podiatrist Dale Feinberg to Crossroads Mission. A vanload of stylish shoes made by the Dr. Comfort diabetic shoe company was presented Wednesday at the women's shelter and will be distributed during the coming weeks.
 |
| Dr. Dale Feinberg and his Wife |
"We are hoping they use these shoes to help increase their cardiovascular fitness, decrease instances of diabetes and help them walk into a better future for themselves and their family," said Feinberg. He said the shoes are specially made for foot problems associated with diabetes.
Source: Chris McDaniel, Yuma Sun [3/10/10]
|
|
|
"A Lot of Options For Patients With Difficulty Tying"
"Orthofeet shoes have been a reliable and consistent part of our diabetic shoe program for over 5 years. As our diabetic shoe program has grown, so has the variety and quality of the Orthofeet brand shoes. Our older patients like the dress style shoes and our more active patients like the new mesh athletic style shoes. I have always preferred the Lycra Velcro Orthofeet shoe for my patients with AFO's and the variety of different closures offered provides me a lot of options for patients with difficulty tying. Overall, I plan on continuing to use Orthofeet shoe for my diabetic patients for a long time to come." Jonathan Moore DPM, MS
Orthofeet Shoes = Superior Patients Care + Better Bottom Line:
Shoes - $45 to $55; Prefab Inserts - $9.95; Custom Inserts - $23; Toe-Filler - $75.00;
Try & compare: Get the first 10 pairs at Half Price!!!
www.orthofeet.com 800-524-2845
|
|
| RETIRED PODIATRISTS IN THE NEWS | |
PA Podiatrist/Aviatrix Receives Congressional Gold Medal for WWII Service
When Mary Reineberg Buchard was growing up in York, PA she would exclaim: "I'm going to be an aviatrix!" The daughter of a shoe store owner studied at Temple University, became a podiatrist and opened a practice in York. She also bought an airplane with other people, learned how to fly, and became a certified pilot in York. She served in the Civil Air Patrol.
 |
| Dr. Mary Reineberg Buchard (Courtesy of Susan Mulins and Eileen McDargh) |
So, when the call came for women to fly military planes in non-combat missions during World War II, Buchard asked her father, Jacob Reineberg, if she could serve her country. He consented, and she gave up her practice. Buchard became one of the "fly girls" who served as Women Airforce Service Pilots, also known as WASPs. The aviators tested planes and ferried them wherever they needed to go.
 |
| Dr. Mary Reineberg Buchard (Courtesy of Susan Mulins and Eileen McDargh) |
They were never considered "real" military pilots, and their service went unrecognized for years. But on Wednesday, the aviators received the Congressional Gold Medal, the highest civilian honor given by Congress, in a ceremony on Capitol Hill. Buchard, 94, lives in a retirement community in southern California.
Source: Teresa Ann Boeckel, York Daily Record [3/10/10]
|
|
| QUERIES (CLINICAL) | |
Query: Recurrent Inferior Calcaneal Ulceration
This patient has recurrent ulcerations of inferior heel despite accommodative AFO and proper footgear. Initial wound resulted in loss of inferior fat pad.
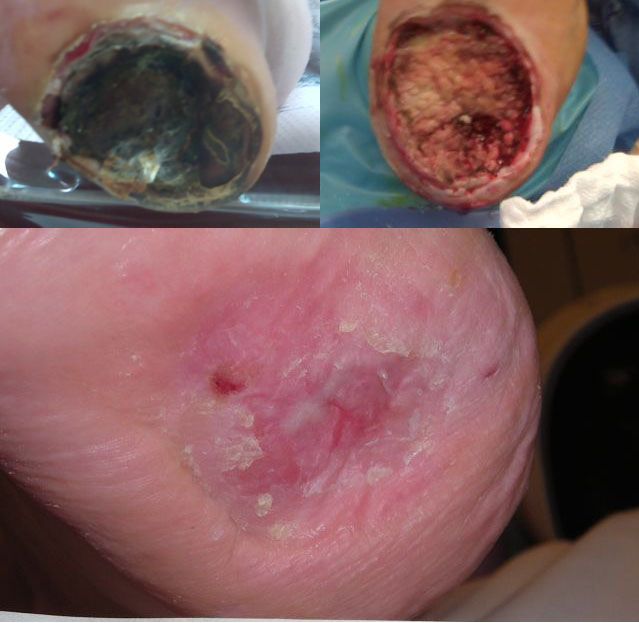 |
| Calcaneal Ulceration (Pre-, Intra, and Post-op) |
Her PMH is significant for spina bifida with resultant partial LE paralysis and profound neuropathy. Minimal plantarflexion strength is present with calcaneal gait. She had a prior BKA of the right leg. Has anyone had experience with implantable or injectable materials to restore/replace fat pads?
Tony Quinton, DPM, Idaho Falls, ID
|
|
| CODINGLINE CORNER | |
Query: Tissue Expansion Coding
I applied Dermaclose on a patient's foot ulcer. The device applies uniform traction about the periphery of the wound to "stretch" and expand the surrounding skin to obtain wound closure.Is there a diagnosis code and billable CPT for such a procedure?
David Sands, DPM, Great Neck, NY
Response: Dermaclose is an excellent modality for chronic ulcerations.
The procedure code is CPT 11960 (insertion of tissue expander(s) for other than breast, including subsequent expansion) and the procedure for removal is CPT 11971 (removal of tissue expander(s) without insertion of prosthesis). In Michigan, however, it is not a covered benefit.
Bruce Kaczander, DPM, Southfield, MI
Codingline subscription information can be found at:
http://www.codingline.com/subscribe.htm
|
|
| RESPONSES / COMMENTS (CLINICAL) | |
RE: Post-op Numbness Status Post EPF (Neal Kramer, DPM)
From: Peter J. Bregman, DPM
With all due respect and admiration to Dr. Jacobs, I think you have to apply Occam's Razor principle here. I think the most likely case is that the lateral plantar nerve was damaged. Whether it was nicked or caught up in scar tissue from hematoma is to be seen. It is unlikely that scar tissue is the problem with this procedure unless a hematoma was created, leading to nerve complications which Dr. Jacobs points out astutely; however, there is no retraction in this procedure. In this case, the symptoms are in the distribution of the lateral plantar nerve, not the medial calcaneal nerve, which rarely, if ever, would feed the lateral heel or distal lateral aspect.
I would certainly not apply any “blame” to this complication; this happens. I think it is a great point that before proceeding with any foot surgery, you should check for nerve pathology, including tarsal tunnel and medial calcaneal nerve entrapment, etc. I also agree that you should closely watch and treat for any potential CRPS-like symptoms, especially if the patient’s psychological profile would predispose them to such a process. Also, I don’t think MRI would be very helpful here, as the damage is so minute that it would likely not be picked up. You could see a hematoma, but an ultrasound exam would do the same. However, you might not get paid for the ultrasound!
Peter J. Bregman, DPM, Tewksbury, MA, footguru@comcast.net
|
|
| RESPONSES / COMMENTS (NON-CLINICAL) - PART 1 | |
RE: Eclinicalworks EMR (Robert Bondi, DPM)
From: Marc Garfield, DPM
eCW is a highly installed product that can be ordered by itself through the company or with a hardware package through Wal-Mart and Sam’s club. It can be used over the Internet or installed in your office. As a billing/schedule EMR combination, the competitors with similar features would be eMDs, Mysis My Way, iMedica, and there are others. It is one of a few products that costs less than $20,000 (initial cost, always get the 5-year cost on your estimate!!!) for a solo practitioner, is CCHIT-certified, Surescripts-certified, and guarantees to...
Editor's Note: Dr. Garfield's extended-length letter can be read here.
|
|
| RESPONSES / COMMENTS (NON-CLINICAL) - PART 2 | |
RE: AAPPM Winter Workshop
From: Jeffrey Kass, DPM
I just got back from the AAPPM's winter workshop in Pittsburgh. If any of my colleagues feel they are going through the "daily grind" and feeling burnt out - I must say that the AAPPM meetings are a great way to "recharge your batteries." The meetings differ from most conferences in that they are not filled with academics per se, but focus more on management. This is something that was not taught at NYCPM, at least when I attended. A second aspect of the meetings was the lack of negativity. There seemed to be an overall lack of complaining, and a more proactive approach of just how to improve your practice. I highly recommend the meetings and organization for everyone.
Jeffrey Kass, DPM, Forest Hills, NY, jeffckass@aol.com
|
|
| RESPONSES / COMMENTS (NON-CLINICAL) - PART 3 | |
RE: Unscrupulous Billing of Routine Care (Dan Klein, DPM)
From: Multiple Respondents
I would like to add my two cents to the ongoing debate of podiatrists who creatively patients who have seemingly good circulation and feet are sensate. I have been practicing for 30 years and I continually rant about this situation. I continually see patients from podiatrists near and far who come to the practice who were creatively billed. We will continue to see these patients because podiatrists fear asking patients to pay for a service because they may go elsewhere. This subject has been discussed ad infinitum, and I don't see things changing. I sometimes feel like I am yelling into a vacuum. To those practitioners who continue to do this, please, please stop doing questionable billing. You may be surprised that patients will pay for services they value.
Sandy Schustek, DPM Charlottesville, VA, sschustek@comcast.net
The "variation" in billing "routine foot care" is more fundamental than a purported failure to follow LCDs. While I agree that integrity can be an issue in some cases, all of the criteria that are considered in whether or not the service is a legitimate claim are relative. For instance, what is "sparse hair growth" in an individual who never had pedal hair? I recall grand rounds where some doctors saw infections, others saw only irritation. Some could palpate pulses, others could not. Are toes cold due to physiology, or environmental conditions of the preceding 15 minutes? Some thought we should amputate, others had more conservative approaches using the same clinical observations. It's medicine and it's imprecise. All of these clinical findings are difficult to prove or disprove, which is why the LCDs regarding routine foot care and onychomycosis have been problematic from the outset.
Shay E. Fish, DPM, San Antonio, TX, fishdpm@aol.com
It is with great interest that I have followed the thread regarding routine foot care. My advice is this... do the exam! One cannot assume that a person does or does not qualify for routine foot care BEFORE entering the patient room. Medicare has set forth the guidelines for routine care and one should let the chips fall where they fall. If a person qualifies for routine foot care and YOU tell them that it is a non-covered service... YOU ARE GUILTY. If the person does not qualify and you tell them that they do.... YOU ARE GUILTY.
There has been more than one case where I have a patient under the care of a vascular specialist, is a diabetic, has no pulses, with dependent rubor, thin frail skin, edema, and thin nails who the "last podiatrist" says needs to pay $45 for their service. Well, that is fraud also, my friend. You are entitled to 11719-Q8 that pays at $17.86 in my area. If you collect the $45 from this patient, you can do some jail time yourself. Truth is ALWAYS the easiest thing to defend. Sometimes, I have found that podiatrists are just choosing which people qualify according to the direction that pays the best. Under-utilization, as well as over-utilization, is a grave injustice to the patient. The definition of integrity... doing the right thing just because it is the right thing.
Karen Malley Banks, DPM, Thomasville, GA, kmbwwjd@rose.net
|
|
| RESPONSES / COMMENTS (NON-CLINICAL) - PART 4 | |
RE: Defeat of Podiatry in NJ Diagnostic Ultrasound Case (Henry Slomowitz, DPM)
From: Larry Cohen, DPM, Ed Davis, DPM
For several days now, I have witnessed the bashing of our podiatric society over the inability to overturn the diagnostic ultrasound issue. As I understand the situation, and please correct me if I am wrong, all diagnostic ultrasounds have to be done in an approved facility. Orthopedists are NOT allowed to do them in the office either. This is another cost-saving measure imposed by an insurance company at the expense of their in-network physicians. The policy is not discriminatory, so do not blame the state society.
Larry Cohen, DPM, Clinton, NJ, larrydpm2002@yahoo.com
I agree that third parties should not deny coverage for services performed within the scope of one's licensure. It is my hope that podiatrists in New Jersey vigorously pursue the situation. It is also important to be pro-active and suggest that we move to create a certification mechanism for podiatric ultrasound. Perhaps we need the assistance of ultrasound suppliers to the profession and an academic institution(s) to help create such a process.
Ed Davis, DPM, San Antonio, TX, ed@sanantoniodoc.net
|
|
| RESPONSES / COMMENTS (NEWS STORIES) - PART 1 | |
RE: Laser Holds Hope for Treating Onychomycosis: (Michael Uro, DPM)
From: Bryan C. Markinson, DPM
I congratulate Dr. Uro and Patholase on attempting to apply scientific evidence to their treatment. However, Dr. Uro's post on the Pinpointe study is somewhat confusing. He refers to a blinded study in which all patients were treated. The study was not "blinded" if the treating doc knew what treatment the patient was receiving. Was there a control/sham arm? The fact that independent physician reviewers do not know who the patients are does not define "blinded."
With regard to the reviewers, "blinded" would mean they did not know if the patient received active or sham treatment. Also, how can a "retrospective" study be reviewed "prospectively"? Finally, if there was no randomization scheme, and all of the cases reviewed by the physician panel were actively treated cases, then it can't be a random review. Basically, this was a retrospective look at a series of cases that was reviewed for efficacy by an independent physician panel. There is nothing wrong with this; it just should not be passed off as a "prospective, randomized, blinded" review.
Furthermore, Dr. Uro does not define "efficacy", a requirement of the FDA. Does he mean mycologic cure, complete cure, or some intermediate step? I do agree with his statement that "There is no device or medication that I am aware of that will provide a permanent cure." Unfortunately, the radio ads for Pinpointe in the New York metropolitan area, occurring almost every fifteen minutes on some days, report 88% cure "once and for all." This seems discordant with Dr. Uro's results of 79% efficacy and his statement that no cure is permanent.
Disclosure: I have been an active advisor to Nomir Medical, makers of the Noveon Laser.
Bryan C. Markinson, DPM, NY, NY, Bryan.Markinson@mountsinai.org
|
|
AAPPM & PM News Present
Practice Management 7-Day Cruise to Alaska
(Following the 2010 APMA Annual Meeting in Seattle) July 18-25, 2010
DON'T GET CLOSED OUT - Register Now
.jpg) |
| Princess Cruise to Alaska |
CLICK HERE FOR FULL BROCHURE
|
|
| RESPONSES / COMMENTS (NEWS STORIES) - PART 2 | |
RE: $1,475,000 Settlement for MD's Failure to Diagnose Charcot Foot (Tip Sullivan, DPM) From: Multiple Respondents
Dr. Sullivan has asked for references in support on my statement that a patient with Charcot's joint disease, absent ulceration or severe deformity, is at no greater risk for amputation than a diabetic patient without a Charcot's joint deformity. Sohn MW., Stuck R., et al. Diabetes Care, 33 (1), 2010; Salan CL., Hagu MI., Zimmerman B., et al. Clin Orthop Rel Res 435, June 2005. I can provide more should you require them.
Perhaps Dr. Sullivan can now provide me with a level 1 or 2 study demonstrating the efficacy of surgical intervention in preventing leg amputation in the patient with Charcot's joint disease.
As we speak, I am caring for several patients with ulcers and terrible infection associated with Charcot's joint disease. One had an IM nail that I did 3 years ago with failed fusion, one never had surgery, one had a large xfix that I did with re-deformity. As bad as all of these cases are presently, I suspect none will result in leg amputation.
Yes, they get repeated ulcers and infections, require expensive care, and lose toes and metatarsals. The issue is leg amputation and NOT other issues which may or may not justify surgery.
Allen Mark Jacobs, DPM, St. Louis, MO, allenthepod@sbcglobal.net
Editor's Note: Extended-length letters by Drs. Douglas Pacaccio and H. David Gottlieb can be read here.
|
|
PODIATRY MANAGEMENT'S AFFORDABLE ONLINE CME
You can Earn 30 CPME-Approved CME Contact Hours Online
Earn 15 Contact Hours for only $139(Less than $14 per credit)
http://www.podiatrym.com/cme.cfm
Choose any or ALL (30 CME Contact Hours) from the 20 CME articles posted
You Can Now Take Tests and Print Your CME Certificates Online
|
|
| CLASSIFIED ADS | |
OFFICE SPACE TO SHARE - NYC
Wanted- Licensed podiatrist to share space in a State-Of-The-Art medical office in the midtown area. Please call Dr. Robert Singer (212) 921-5775 or e-mail dr.roberth.singer62@netzero.net
FULL-TIME PODIATRY OPPORTUNITY - BOSTON, MA
HealthDrive is seeking a caring podiatrist to join our group practice. We currently have a FT non-surgical opportunity available in the Boston, MA area. We offer a competitive salary, Paid malpractice Insurance, health and dental Insurance, long & short term disability, flexible schedule (No weekends), established patient base, equipment, supplies and complete office support provided. If interested in this opportunity, please call Maria Kelleher (toll free) at 877-724-4410 or email caring@healthdrive.comASSOCIATE POSITION - CONNECTICUT
Associate needed full or part-time for Nursing homes in Connecticut. Need hard-working, ethical individual. Must have CT license. Excellent salary. Please call Zina (347)307-4333 for additional information.
ASSOCIATE POSITION - TAMPA BAY
Associate needed for a dynamic multi-doctor practice in the Tampa Bay area. Preference given to a PSR 24+ training and must have a Florida license. Well-established practice, high-tech with EMR and digital x-rays, with specialties in sports medicine, surgery and wound care. No nursing homes or HMOs. Excellent hospital privileges available. Choose an area of practice concentration that you are passionate about and enjoy a lifestyle for yourself and your family second to none. Kindly forward C.V. to e-mail drcosentino@tampabay.rr.com
ASSOCIATE POSITION - DAYTONA BEACH, FLORIDA
Associate position with buy-in potential. Daytona Beach, Florida Great opportunity for PSR 24-36.trained physician to join state-of-the-art practice. Please forward resume to pfk4@yahoo.com
ASSOCIATE POSITION-INLAND EMPIRE, SOUTHERN CALIFORNIA
Associate needed full or part-time for multi office practice. Must be ABPS BC/BQ. Hard working, ethical individual who is looking to a possible partnership opportunity. Looking for current licensed or resident completing program this spring. Email CV to bkatzman2@earthlink.net or call Martha 909 984-5614.
ASSOCIATE POSITION - SAN FRANCISCO, CALIFORNIA
We’re seeking an energetic and enthusiastic Associate to help our thriving non-surgical practice grow. We provide state-of-the-art sports medicine, trauma and lower extremity care. Excellent compensation package. Visit our website to apply.
HOME FOOT CARE PHYSICIAN NEEDED - LOS ANGELES, CALIFORNIA
Honest, caring, hard-working podiatrist needed to make visits to homebound patients, facilities, etc. for Home Foot Care, Inc. Part time position, flexible hours, independence and excellent compensation. If interested email CV to homefootcare@hotmail.com
ASSOCIATE POSITION - NORTHERN VIRGINIA/DC SUBURB
Excellent associate practice opportunity leading to partnership for PSR 24-36 foot and ankle surgically-trained physician. Currently 4-doctor/2 office practice in fast-growing area, expanding to 5 doctors. Hard working, personable, highly-motivated individuals needed. Great opportunity with excellent salary and benefits. No nursing homes. Top hospitals. Fax CV with references to 703-491-9994
ASSOCIATE POSITION (PART–TIME) WHITE PLAINS, NY
Part-time associate wanted for busy 22 year old White Plains office. Call 914-325-9198 for further details.
PRACTICE FOR SALE - FLORIDA CENTRAL/SOUTH
Turn-key operation grossing $570,000 annually based on one full-time doctor. Great opportunity for growing the top-line. Surgery is only 14% of the professional man-hours; it can significantly increase income. Medicare makes up 64% of revenues. Seller will assist with transition. Call 863-688-1725, ask for Chas.
PRACTICE FOR SALE – CONNECTICUT
Outstanding practice for sale in northern Fairfield county, CT. Shared space with other medical professionals. Very low overhead. Grossing almost $300K on 30 hours per week. Referrals from three different primary care physician offices. If interested e-mail CTPodiatry@gmail.com
PM News Classified Ads Reach over 12,000 DPM's and Students
Whether you have used equipment to sell or our offering an associate position, PM News classified ads are the fastest, most-effective way of reaching over 12,000 DPM's. Write to bblock@podiatrym.com or call (718) 897-9700 for details. THIS OFFER DOES NOT APPLY TO BUSINESSES PROVIDING PRODUCTS OR SERVICES. Note: For commercial or display ads contact David Kagan at (800) 284-5451
|
| Disclaimers |
Acceptance and publication by this newsletter of an advertisement, news story, or letter does not imply endorsement or approval by Barry Block or Kane Communications of the company, product, content or ideas expressed in this newsletter. Podiatric Medical News does not represent the views, and is a separate entity from Podiatry Management® Magazine and Podiatry Management® Online. Any information pertaining to legal matters should not be considered to be legal advice, which can only be obtained via individual consultation with an attorney. Information about Medicare billing should be confirmed with your State CAC.
THIS MESSAGE IS INTENDED ONLY FOR THE USE OF THE INDIVIDUAL OR
ENTITY TO WHICH IT IS ADDRESSED AND MAY CONTAIN INFORMATION THAT IS
PRIVILEGED, CONFIDENTIAL AND EXEMPT FROM DISCLOSURE.
If the reader of this message is not the intended recipient or an
employee or agent responsible for delivering the message to the
intended recipient, you are hereby notified that any dissemination,
distribution, or copying of this communication is strictly
prohibited. If you have received this communication in error, please
immediately notify me and you are hereby instructed to delete all
electronic copies and destroy all printed copies.
DISCLAIMER: Internet communications cannot be guaranteed to be
either timely or free of viruses.
| | Guidelines |
- To Post a message, send it to: bblock@podiatrym.com
- Notes should be original and may not be submitted to
other publications or listservs without our express written
permission.
- Notes must be in the following form:
RE: (Topic)
From: (your name, DPM)
Body of letter. Be concise. Limit to 250 words or less). Use
Spellchecker
Your name, DPM City/State
- Subscribers are reminded that they have an ethical obligation to disclose any potential conflicts of interest when commenting on any product, procedure, or service.

| |
|
Browse PMNews Issues
Previous Issue | Next Issue
|
| |

|
|
|