



|

|
|
|

|
Search
09/06/2022
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Gene Test for Bunions
From: John Moglia, DPM
I am often asked by patients if they will develop bunions as their parents and grandparents did. There is a genetic test readily available and provided by 23 and Me. I took the test by spitting into a test tube and paid the $99 fee. The test results confirmed my Western European history as well as no susceptibility to the uncommon medical disorders listed on their website.
Incidentally, I was relieved to learn that I do not have the dreaded genetic code for bunions, but sadly the test confirmed my lactose intolerance.
John Moglia, DPM, Berkeley Hts, NJ
Other messages in this thread:
04/29/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Kudos to Amerx
From: Ted Mihok, DPM
Our Coupeville Central Lion's Club had a successful trip last month to Mexicali, Mexico. We delivered medical supplies to the most vulnerable people in Mexicali. I especially want to thank the Amerx Corporation for their contribution of wound care items. Amerx has been a sponsor of our International project for years. They continue to give back, and focus on our Lion's club motto of "WE SERVE".
Ted Mihok, DPM, Alameda, CA
04/28/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Diogenes the Cynic
From: Rod Tomczak, DPM, MD, EdD
Diogenes is partially famous because he spent time carrying a lantern looking for an honest man. He is also called Diogenes the Cynic. A good 30 years ago, I shared some uninhibited conversation and a cup of coffee with Leonard Levy, DPM, the Dean of the Des Moines college. I was a couple of classes into pursuing my education doctorate and we talked about the significance of a doctorate in education as a podiatrist in academia. In a moment of astonishing frankness, Leonard said to me, “I could do so much better for myself if I only had an MPH from Columbia and not a DPM accompanying it.”
I had experienced a taste of the three-tiered medical caste system where MDs were on top, DOs made up the second class, then there were the rest of us who made up the third layer. It was impossible to “tier up” with a DPM degree. The graduation stole, as part of our academic...
Editor's note: Dr. Tomczak's extended-length letter can be read here.
04/23/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
From: James Hatfield, DPM
The post by Louis Profeta, MD is excellent and should be required reading by all residents, students, and applicants. I'm so tired of hearing all the whining going on about our profession. We have an excellent future and waste too much time obsessing about our degree. Get a life!
James Hatfield, DPM, Encinitas, CA
04/14/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Podiatry’s Identity Crisis
From: Arden Smith, DPM
Background: this is my third winter since retiring and snow-birding. Both my former partner and I are both double boarded and we were lucky enough to have developed a very early niche in the medical and surgical treatment of the high-risk diabetic foot and limb salvage through having a satellite office within a large endocrine practice, beginning in the mid-1980s. This was something that we had very little training for and learned by the seat of our pants and attending diabetic foot conferences. We started out asking a friendly vascular surgeon if we could assist on referred cases and over a relatively short period of time, started asking him if he wanted to assist us; and then eventually stopped asking, other than the vascular consult. We also had a large volume general podiatry practice that was somewhat surgically oriented. We would see multiple generations in families.
Our general practice was a neighborhood practice in a middle class area, and our diabetic practice was a referral hub between two...
Editor's note: Dr. Smith's extended-length letter can be read here.
04/09/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Podiatry Salaries vs. Nurse Salaries from Becker's Hospital Review
From: Steven D Epstein, DPM
Certified registered nurse anesthetists (CRNAs) make more than most of us do. An RN makes this after only four years of undergraduate education. And this doesn't preclude them from going into advanced practice; in fact, experience as a "mere" RN is usually required to be accepted for advanced practice training. Failing to be accepted for that consigns one to a miserable six figure salary career.
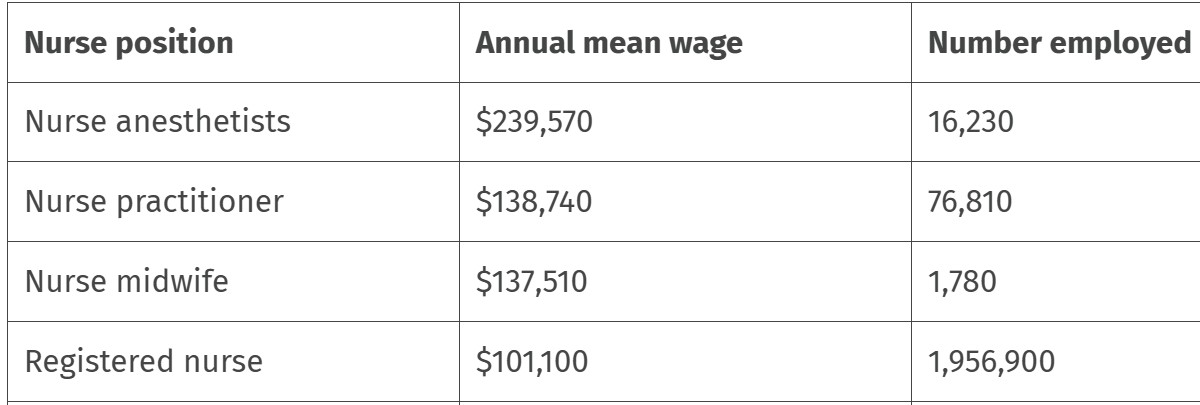 |
Nurse's Salaries (Source: Becker's Hospital Review) |
This kind of info is now freely available for high school and college students to see. Is it any wonder that smaller numbers of students are choosing podiatry as a career?
Steven D Epstein, DPM (retired), Lebanon, PA
02/26/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
From: Lawrence Rubin, DPM
Along with others posting, I was saddened to hear that APMA has fired two very qualified and seasoned health policy employees. I hope there is justification for this, since national health policies having to do with health insurance reimbursement are changing dramatically with the advancement of the Medicare led value-based care payment model. APMA health policy employees should be thinking forward and hard at work developing ways and means to help its members transition to value-based care now, as it is already moving forward and is considered the future of healthcare to be fully implemented in 2030.
Value-based care offers numerous benefits for both patients and providers. These benefits include improved patient outcomes, greater physician satisfaction, and a more sustainable financial model by focusing on quality of care rather than just volume of services delivered. It also offers financial rewards for those podiatrists who will collaborate in providing lower extremity chronic disease prevention services.
APMA members who delay the transition due to lack of information and guidance could potentially be missing opportunities for better patient care and could put their practices at a competitive disadvantage. Hopefully, this was considered when the decision to fire these employees was made.
Lawrence Rubin, DPM, Las Vegas, NV
02/25/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Shocked and Saddened
From: Mark Block, DPM
On February 21st, out of the blue, I, along with the APMA membership, was informed of significant changes within the Association. It appears that APMA has decided to undergo a major restructuring.
Having been a long-standing member since my time as a student, I recognize that while other podiatric entities contribute meaningfully to our profession, APMA along with other missions serve as a unifying voice. Its ability to lobby and advance legislative initiatives is essential to the profession’s strength and future. I have come to appreciate that the Association’s long-term viability must be ensured. Should APMA cease to exist, it would leave a tremendous void with serious negative ramifications...
Editor's note: Dr. Block's extended-length letter can be read here.
02/24/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1C
From: Irv Luftig, BSc, DPM
Stephen Peslar is correct that many of the chiropodist graduates have left the profession, and the actual DPM podiatrist population is dwindling because of the idiotic 1993 legislation, stopping any DPM podiatrists coming into Ontario from practicing their full scope. This was a power grab by the medical establishment and an extremely poorly thought-out attempt by the government of the day to bring in chiropody practitioners to work in nursing homes and hospital clinics on a salary. The right to establish themselves as private practitioners and make positive progress in Ontario was through a charter of rights challenge brought by the chiropodists in the late 1980s which was successful. The governing college for the profession has been fighting tooth and nail for many years to establish podiatry as a properly recognized profession and unify us and increase our scope of practice to a full scope.
I personally had a wonderful and fulfilling career as a DPM podiatrist in Ontario until my retirement. There are many excellent, hardworking chiropodists and many excellent, well trained, skilled podiatrists in Ontario who have been pioneers in surgical procedures and...
Editor's note: Dr. Luftig's extended-length letter can be read here.
02/24/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1B
From: Daniel Chaskin, DPM
There has got to be some sort of educational program so non-surgical podiatrists can increase their scope of practice to treat the ankle as well as the rest of the body. Nursing schools should offer advanced placement for DPMs who wish to medically treat the ankle and above, as well as systemic diseases in certain states. This way, a DPM could qualify to get a nursing degree as a path to obtaining a license for treating the ankle as well as systemic diseases.
Once getting a nursing degree, they could then opt to get a nurse practitioner degree. Is it possible Touro might consider offering advanced placement for DPMs to obtain a nursing degree as a path to increasing scope?
Daniel Chaskin, DPM, Ridgewood, NY
02/24/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1A
From: David Secord, DPM
Although I agree that the future of the profession is plenary licensure, I’m confused as to why there would be a push to obtain a degree as an osteopath with a podiatric sub-specialty, as opposed to obtaining a degree as an allopath with a podiatric sub-specialty? There are a certain finite number of medical theories out there, including allopathic, osteopathic, homeopathic, chiropractic, native American Indian pan-theistic naturopathy, witch doctors, Eastern Indian Ayurvedic medicine, and a few others.
Allopathic medical theory has as its basis the idea of pathology from disease state: bacteria, virus, spirochete, genetic dyscrasia, prion, etc. Unless I missed something critical in medical school, that’s the disease model we in podiatry follow as well. As such, podiatric medicine IS allopathic medicine. As we don’t follow the osteopathic theory of medicine, why would we obtain degrees as osteopaths, practice as allopaths, and so muddy the waters? I’m finding this very curious.
David Secord, DPM, McAllen, TX
02/21/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1B
From: Stephen Peslar, BSc, DCh
Dr. Tomczak was correct when he wrote there are about 600 chiropodists for about 15 million people in Ontario, Canada. Decades ago, Ontario Ministry of Health decided to shut down podiatry based on some unfortunate foot surgery outcomes performed by podiatrists. In 1991, the Chiropody Act was passed with the clause, “No person shall be added to the class of members called podiatrists after the 31st day of July 1993.”
Then in 2015, the Health Professions Regulatory Advisory Council completed an extensive study of over 350 pages, that included a jurisprudence review and a consultation with stakeholders. The concluding recommendation to the Minister of Health was, “no changes should be made at this time to the current legislation on the registration of podiatrists in Ontario.” Since 1983, there have been about 900 graduates from the Ontario chiropody program. Around 300 have abandoned the chiropody profession mainly due to...
Editor's note: Stephen Peslar's extended-length letter can be read here
02/21/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1A
From: Rod Tomczak, DPM, MD, EdD
I ask everyone who replied to this week's survey concerning options for undergraduates interested in healthcare to read my extended letter concerning the possibility of a DO degree and a commitment to foot and ankle care without a DPM degree. The PM News of 02/15/2025 and 02/17/2025 are intrinsically attached to the survey and the current DPM population.
It is important that everyone who participates in the survey understands this could be the end of the DPM degree and podiatry since there will not be a podiatry degree but merely a new medical/surgical specialty called podiatry. Although APMA could exist just like the AAOS exists, APMA would not be the same organization.
Rod Tomczak, DPM, MD, EdD, Columbus, OH
02/20/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1C
From: Stephen Peslar, BSc, DCh
While Dr. Seuferling views a foot nurse issue as an opportunity not a threat, in Canada they will have a conference that will include these topics: MedFlex nail restoration, Onyfix nail correction, onychomycosis diagnostics and photodisinfection, SWIFT wart removal, proper footwear, padding and off-loading, pedorthic management, Vandenbos procedures, heel pain that could be something else, not plantar fasciitis, and "Rash: a review of dermatitis, infections, and suspicious skin lesions."
Another nurse’s foot care association in Canada states, “our members have obtained the knowledge, skill, and judgement to competently provide medical foot and lower limb care… to determine which orthotic devices will improve one’s overall health and wellness. Our members have the option to consult with laboratory technicians who are qualified HCPs who specialize in the design and build of orthotic devices.”
It appears that they want to do more than trim toenails, reduce plantar calluses, and enucleate IPKs. If they’re doing this in Canada, my guess is they’re doing the same or soon will be performing SWIFT wart treatments, performing OnyFix nail correction, performing the Vandenbois procedures, and casting (or scanning) and dispensing orthotics.
Stephen Peslar, BSc, DCh, Toronto, Ontario
02/20/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1B
From: Chris Seuferling, DPM
Point of Clarification: I’ve received comments about “what a podiatrist SHOULD be”. The intent of my post was not that I agree with the current podiatry residency training model, but rather how we should deal with the existing gap of traditional podiatric care IF the current residency model remains as is. These are two intertwined, but different topics.
Bottom line: I would love to have podiatry satisfy all the general foot care needs (nail, callus, diabetic, etc.) of the population. I feel we have lost our identity as to what podiatry “SHOULD” be and residency program revision needs to be a topic of discussion at the table. However, if that’s not an option and it is truly a “bridge too far”, then we need to deal with the reality that IS, not the “SHOULD” be.
Chris Seuferling, DPM, Portland, OR
02/20/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1A
From: Ivar E. Roth, DPM, MPH
I agree with Dr. Feinman. It does appear that today’s graduates look to lifestyle and convenience as their priorities. I remember when I was so thirsty for knowledge. The competition to get a residency, which only 50% of the class got was what caused us all to be very competitive. Now everyone is guaranteed a residency and so complacency seems to have taken hold with a good number of the graduates.
I have recently interviewed candidates for an associate position, and I can tell you most of them are just looking to work the bare minimum 40 hours a week with no intention or drive to work more hours or harder than the minimum required. Needless to say, I have been disappointed.
Ivar E. Roth, DPM, MPH, Newport Beach, CA
02/19/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1C
From: Ross B. Feinman, DPM
I have been practicing for over 22 years; I have seen the ups and downs of the profession as well as the residency programs. I have been fortunate enough to be involved with podiatric students through the various programs at multiple hospitals, and I have worked with some very talented residents through the years as well as students! In previous years, students were hungry for knowledge, enjoyed the banter of being “pimped”; they knew it was for educational purposes, not a personal vendetta against them. They also came prepared for the case, knew the basics and seemed interested.
Unfortunately, today many students now want to be done by 5 PM, not show up, or have to take their dog to the vet. The idea of this as a lifelong profession seems to have become lost in the fog as many students today seem to be more interested in dinner time than...
Editor's note: Dr. Feinman's extended-length letter can be read here.
02/19/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1B
From: Glenn McClendon, DPM
We all get tired at times of trimming toenails and calluses, but don't other doctors get tired of their most routine treatments. Why don't podiatrists have a non-insurance nail segment of their business for many of the patients who don't meet qualified at-risk foot care. It could be an adjoining or simultaneous adjunct to your office. A trained nail tech could do that work and take a load off of you. And it would be all cash. Ophthalmologists employ optometrists. ENTs employ audiologists. Almost all MD/DOs have a practitioner working under them. It would be a way to produce income from others’ efforts, and provide a good referral source.
It would be great to have some income when on vacation. I'm sure there are plenty of people who would prefer to go to a nail salon affiliated with a podiatrist vs. one in a local shopping center for various reasons. How many podiatrists sell OTC products through their office for income and convenience to patients? Are there challenges in making this an extension of your medical practice? Sure. Rarely is there any easy money without some sacrifice. Maybe someone will come up with a business model along these lines that will work. I'd sure consider it.
Glenn McClendon, DPM, Conway, AR
02/19/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1A
From: Elliot Udell DPM)
We need to be honest with ourselves. Comparing our profession to dermatology and orthopedics to show that there is nothing wrong with teaching nurses how to practice general podiatry is unfair. Why? Every dermatologist and orthopedic surgeon knows that the overlap between what we do and what they do in their practices is small. We do not operate on knees and hips nor treat skin disorders above our anatomic ranges of practice. On the other hand, everything a podiatrist does can be duplicated by someone in the MD and DO worlds.
I suspect that Dr. DiResta's concern is that MDs and DOs choose not to practice non-surgical general podiatry. If we train nurses to do what almost all of us do most of the time, why would they send us any of their patients for foot care? They can hire a nurse to render all general foot care and profit from it. Taking it one step further, nurses and PAs can be trained to do most of the foot surgeries we do, but we probably don't have to worry about that in a few years to come.
Elliot Udell, DPM, Hicksville, NY
02/18/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Let’s Not Abandon Routine Foot Care
From: Lawrence Rubin, DPM
So many podiatrists are abandoning providing what is often time-consuming and poorly reimbursed but potentially limb-saving "routine foot care." Shouldn't we continue to own this often humanitarian service by doing what Dr. Fones did?
Dr. Fones was a dentist in Bridgeport, Connecticut. In 1913, he trained his assistant, Irene Newman, to be the first dental hygienist. That led to them founding dental hygiene education in the United States. How about getting APMA to work towards accomplishing this with the stipulation that supervision by a podiatrist be mandatory in every state.
Lawrence Rubin, DPM, Las Vegas, NV
02/17/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: The Wonder Bread Solution
From: Rod Tomczak, DPM, MD, EdD
There seem to be two recurring and interconnected questions on PM News lately. First, why is enrollment in colleges of podiatric medicine declining and secondly, why is there a push to increase the scope of practice to include the prescribing of systemic medications that do not directly affect the foot? Surprising as it may sound, the two may be closely associated.
When pre-med major students, not pre-podiatry majors, came to Des Moines to interview for the podiatry program, we stressed the fact that if they came to Des Moines, they would be completely integrated with DO students for their classes. Same lectures, same teachers, same time, same room, same exams. They could team up with DO students for study groups and had identical printed class notes approved by the lecturer and supplied to both DO and DPM students by the note service before...
Editor's note: Dr. Tomczak's extended-length letter can be read here.
02/15/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: $250,000 Challenge to Podiatric Medical Schools
From: Sev Hrywnak, DPM, MD
I am writing to express my strong belief that for podiatry to thrive in the future, it is essential to establish a full license that reflects the comprehensive training in this field. To achieve this, we must invest in podiatric medical schools that offer the necessary courses and clinical rotations at teaching hospitals.
I have had the pleasure in teaching the past 27 years, 3,611 podiatric medical students, 1,490 allopathic medical students, and 477 osteopathic medical students. The data shows that in order to keep a high applicant pool to podiatric medical schools and to keep pace with healthcare providers in mainstream medicine, i.e., physician associates and nurse practitioners who have a full license, podiatric physicians should have a full license.
I am committed to supporting this vision and will personally donate $250,000 to a podiatric medical school that prioritizes a curriculum and practical experiences in teaching hospitals leading to a full license (plenary license). This investment aims to foster a new generation of highly skilled podiatric physicians who can elevate the profession and ensure its relevance in the evolving healthcare landscape. The goal is to have this in place by 2026. Let us work together to create a future where podiatry is not only respected but also essential in patient care.
Sev Hrywnak, DPM, MD, Chicago, IL
02/13/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
From: Vince Marino, DPM
Vince Marino, DPM, Novato, CA
02/12/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: American Foot Care Nurses
From:James DiResta, DPM, MPH
If you are thinking of surviving on the delivery of routine foot care, you have some very serious competition out there and it's growing. https://www.afcna.org/
James DiResta, DPM, MPH, Newburyport, MA
02/07/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
From: Ivar E. Roth, DPM, MPH
Dr. Rubin has hit this nail on the head. All we need is a group of “thought leaders” to come up with some solutions here. I do not feel it is the APMA that we should turn to. If they have not done this to date, there is a reason. I believe we need some real “in the trenches” DPMs with experience in life, and I for one, would volunteer to help out. We have so many problems going on concerning our future.
I recently spoke with a recent residency graduate who did a three-year surgical program, and he said no one from his program ever did a case skin-to-skin in the three years of training. How is this possible? He said he is too afraid to say something as he is early on in his career and does not want to make any problems. I am just dumbfounded that no one has spoken up. If others reading this post are moved to be part of the “thought leaders” let’s hear from you and hopefully we can do something positive together.
Ivar E. Roth, DPM, MPH, Newport Beach,, CA
02/06/2025
RESPONSES/COMMENTS (NON-CLINICAL) - PART 1
RE: Where are Our Thought Leaders?
From: Lawrence Rubin, DPM
Recent posts in PM News have made it clear that podiatrists are not the only providers competing for business in today's new foot healthcare marketplace. There are at least a dozen other professional and business entities vying for a piece of the foot care dollar. If our thought leaders do not come forward and recognize this, and if they fail to take swift actions to make sure podiatrists are the preferred providers of all the values included in value-based foot care, the future of our profession will be perilous. I have brought this to the attention of the APMA but so far, no response.
Lawrence Rubin, DPM, Las Vegas, NV
|
| |

|
|
|

