



|

|
|
|

|
Search
07/20/2020
RESPONSES/COMMENTS (CLINICAL) - PART 1
From: David Secord, DPM, Bryan C. Markinson, DPM
I’ve been using the Panacos graft and the bleomycin treatments ever since I first started practicing. I list these two together because they attempt to accomplish the exact same thing with somewhat different techniques.
Bleomycin technique: The bleomycin treatment is my primary treatment for verrucae vulgaris lesions and I currently have a 99.7% success rate over 8 years and hundreds of cases with the added benefit that if the person has multiple verrucae, treating just the one lesion will allow resolution of all...
Editor's note: Dr. Secord's extended-length letter can be read here.
The Panacos procedure was debunked 40 years ago. Search that procedure and you will not find one credible publication about it in any literature.
Bryan C. Markinson, DPM, NY, NY
Other messages in this thread:
05/19/2025
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: David Secord, DPM
Some years back, I was treating a border patrol agent who caught a Mesquite tree thorn in her thumb. She was “treated” at the E.R. and was still having problems. Why? Upon examination, the thumb was about twice the expected diameter—indicating that a foreign body was still present—and the incision made was closed with 2.0 Ethibond. In this case, an examination of the procedure revealed that this was not done by a doctor, nor a PA. Not done by a NP either. This atrocity was committed by an MA. They had a medical assistant (who, rather obviously has zero qualifications or permission to perform a surgical procedure on anyone) inject, incise, poke around, not find, and suture with totally inappropriate material a foreign body procedure.
I don’t know if this relates to the hernia procedure, but one never knows. I recently inherited a patient post-hallux amputation procedure who was told (and given written instructions) that he could immediately start bathing the site, still sporting the nylon sutures. I don’t know if I’ve missed something new, but the “go ahead and bathe immediately post-op” idea isn’t supported by any science and is strongly opposed as far as I’m aware. There is some questionable stuff out there.
David Secord, DPM, McAllen, TX
04/24/2025
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: David T. Weiss, DPM
The effective concentration of dextrose is 50% (hyperosmolar).
Mechanism of Action of Dextrose:
1. Localized Inflammatory Response Dextrose solutions (typically hyperosmolar) act as an osmotic irritant when injected into entheses, ligaments, tendons, or joint capsules. This mild irritation triggers a controlled, localized inflammatory response.
2. Stimulation of Fibroblast Proliferation The inflammatory response recruits fibroblasts to the site of injection.
Fibroblasts are key cells responsible for collagen synthesis. This process promotes:
o Neocollagenesis....
Editor's note: Dr. Weiss' extended-length letter can be read here.
04/24/2025
RESPONSES/COMMENTS (CLINICAL) - PART 1A
From: Ron Werter, DPM
My suggestion is to take a course and get certified. Don’t screw around with it. The least you can do is be ineffectual, the worst is to cause damage.
A close friend of mine is an MD whose practice is exclusively prolotherapy. After 20 years doing this, he is still taking additional courses. I asked him about my doing this in my practice for heel pain. "Sure," he said, "but take the course. It’s not as simple as you think."
Ron Werter, DPM, NY, NY
03/03/2025
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: Gary S Smit, DPM, Elliot Udell, DPM
I have seen this as a side-effect of medications. This is anecdotal, but I've seen it with anxiety medications like Zoloft and I saw it once as a side-effect from an artificial insulin product. This is very frustrating to treat. I think that oral antifungals is a good idea.
Gary S Smit, DPM, Kme, PA
I recommend doing the biopsy because if it turns out to be psoriasis or some other autoimmune disease, there are great new drugs available that can address these issues.
One patient of ours had psoriatic plaques all over his body. He went from dermatologist to dermatologist for years and still suffered. Finally, he was placed on Skyrizi and within a short period of time, he had resolution of all of his plaques and feels like a new person. Please let all of us know what the final diagnosis turns out to be.
Elliot Udell, DPM, Hicksville, NY
03/03/2025
RESPONSES/COMMENTS (CLINICAL) - PART 1A
From: PM News Subscriber, David P. Luongo, DPM
This is a picture of my patient with T-cell lymphoma. A biopsy of your patient may be a good idea.
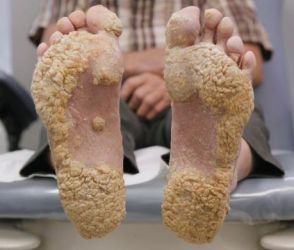 |
Plaque-Like Calluses on Weight-Bearing Surfaces |
PM News Subscriber
I've seen this before. For my patient, it was the onset of menopause where there was a sudden change in hormones. Have that checked out.
David P. Luongo, DPM, Paramus, NJ
12/11/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1
From: Ivar E. Roth DPM, MPH, Jeffrey Kass, DPM
It is possible but first you must get rid of the fungus. Sometimes you may have to use ½” paper tape at the distal end of the toe to hold down the soft tissue. I am trying something new and that is applying a KeryFlex nail to put pressure on the distal tip to flatten out as the nail grows over. I will report on if this works. Plan on treating for an extended period of time as these nails are difficult to convert to “new nails”, but I have done it on occasion.
Ivar E. Roth DPM, MPH, Newport Beach, CA
I thank Dr. Weiss for linking us to his informative and very well written article on onychocrptosis and subungual exostosis. I am not sure how often the abnormal nail is a result of abnormal distal phalanx, but the intimate relationship he brings up is certainly of clinical value. Good job.
Jeffrey Kass, DPM, Forest Hills, NY
08/09/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: Paul Kesselman, DPM
Kudos to Dr. Pressman for pointing something out which I have been preaching for my over 40+ years as a clinician. I first came aware of non-invasive vascular technology back in the late 1970s and early ‘80s during my undergraduate medical education at rotations at various VA hospitals in the Chicago area. In those days, the machines were big, bulky, and took up an entire room. Their costs and size relegated them mostly to large clinical or research facilities.
With computer technology, eventually the machinery got more sophisticated and totally paper free and can integrate directly into your computer and eventually into your patient's EMR. Most cost 1/3 of what digital x-rays cost, with many fitting into your briefcase. The current machinery can combine pulse volume recording and photoplethysmography, which are far more sophisticated than...
Editor's note: Dr. Kesselman's extended-length letter can be read here
08/09/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1A
From: Jeffrey Kass, DPM
I’d like to thank Dr. Pressman for the free pearl. I sincerely appreciated the pearl and was ecstatic for the first time someone was not trying to extract money from me. I have also come across patients with palpable pulses who have had stenosis or occlusions and the pearl he has shared is of utmost value.
Jeffrey Kass, DPM, Forest Hills, NY
05/01/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1B
RE: Functional Hallux Limitis
From: Howard Dananberg, DPM
Howard Bonenberger mentioned in a post last week that one of my lectures on functional hallux limitus (FHL) inspired him to treat patients with chronic postural complaints. I appreciate his comments and am glad he was able to find these concepts valuable. I have written extensively on FHL over my career, and have come to the realization that this concept remains misunderstood. The reason why it can impact postural form lies in the following principle. Once the hallux makes ground contact during any step, IT DOES NOT MOVE AGAIN UNTIL TOE-OFF. ln any form of hallux limitus (structural or functional), what is restricted is not the hallux, but the remainder of the foot and proximal structures all the way to the neck.
As the body adjusts for these motions, various sites are stressed repeatedly during each step cycle. And since these motions are repeated thousands of cycles per day, the stress becomes a chronic irritant. In particular, loss of MTP joint motion restricts heel lift, shortens stride length, and causes the ensuing swing phase to be altered in such a way as to make toe-off mechanically inefficient. Since the iliopsoas is the primary hip flexor at toe-off, and originates directly from the lumbar spine, it becomes the site of pain. The references for this are below.
Howard Dananberg, DPM
05/01/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1A
RE: Functional Hallux Limitis
From: Jeffrey Trantalis, DPM
Howard Bonenberger, DPM hinted about a very important and prevalent condition that is seen in many, if not all, podiatry offices. This is hallux limitus. In the early 1980s, I had a professional NFL receiver come to me with hallux limitus. It was obvious that conservative treatment was the only option. At that time, orthotics with a hallux extension was the recommended treatment. So I tried this very treatment, knowing it would probably fail. Well it did fail.
At that time, I dispensed an orthotic where I increased the ability to plantarflex the first metatarsal by supporting the 1st metatarsal-cuneiform joint. This allowed for a more normal function of the first MPJ. This was very successful treatment that allowed the receiver to make his route maneuvers.
Jeffrey Trantalis, DPM, Delray Beach, FL
03/13/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1
From: David T Weiss, DPM
The most powerful way to manage DPN, (besides glycemic control,) is refraining from sugar (and carbohydrates) completely - especially after dinner. Sugar is extremely inflammatory. I have recommended liposomal glutathione (powerful antioxidant) as a supplement, along with L-methyl folate vitamins.
David T Weiss, DPM, Richmond, VA
02/27/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1 A
From: Robert Scott Steinberg, DPM
Not only are there too many schools, but the curriculum has not kept up to the standards for today's podiatric physicians and surgeons to become successful in practice. Colleges are not teaching the courses necessary for podiatrists to sit for the USMLE board exams, keeping the profession under the hallux of others. I suspect the first podiatric medicine college offering a better curriculum will get far more applicants. Let the race begin.
Robert Scott Steinberg, DPM, Schaumburg, IL
02/12/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1 B
From: Khurram Khan, DPM
Small fiber neuropathy (SFN) and large fiber neuropathy (LFN) represent two distinct categories of peripheral neuropathy, differentiated by the size of the nerve fibers they affect and the resultant symptoms and diagnostic approaches. SFN targets small myelinated Aδ fibers and unmyelinated C fibers, leading to symptoms like burning, tingling, and is diagnosed through hstory/clinical evaluation. LFN affects large myelinated fibers responsible for proprioception and vibration sensation, and with diagnosis typically achieved via physical exam and confirmed with nerve conduction studies and electromyography (EMG). The patient mentioned seems to have SFN. The causes of small fiber neuropathy (SFN) include:
Diabetes, autoimmune diseases (e.g., Sjögren’s syndrome, lupus, rheumatoid arthritis, celiac disease), infections (e.g., Lyme disease, HIV, hepatitis C), vitamin deficiencies (particularly vitamins B12, B6, and E), alcoholism, toxic exposures (e.g., chemotherapy drugs, heavy metals, industrial chemicals), hereditary disorders (e.g., hereditary sensory and autonomic neuropathies, Fabry disease), idiopathic (no identifiable cause), and finally metabolic disorders (e.g., thyroid dysfunction, amyloidosis)
Khurram Khan, DPM, Philadelphia, PA
02/12/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1 A
From: Lawrence Rubin, DPM, Bruce I Kaczander, DPM
The sensory dysfunction referred to by Dr. Teitelbaum is called "paresthesia." I have had some patients even complain of a feeling of "bugs running up and down my feet and legs" and similar sensations. Here is more information: Paresthesia: When to pin down a cause.
Lawrence Rubin, DPM, Las Vegas, NV
In my 42 years of practice, I saw patients daily whose neuropathic symptoms were spinal in origin (stenosis, L 4-5, S-1 disc)… it can oftentimes present initially as same, without the patient having current spinal symptoms. They also may have a history of same years ago.
Bruce I Kaczander, DPM, Southfield, MI
01/18/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1 B
From: Richard D Odom, DPM
I suspect the patient is a smoker. If so, his smoking is likely the etiology or cause of his lesions. The reason is because smoking/anxiety can cause these in areas of the body where there are an abundance of sweat glands, plantar foot & palms of hand. This increased moisture leads to some of the glands being over productive and can cause blockage of the surface of sweat gland. Farther production moisture is unable to escape from the gland, leading to increased hyperkeratotic build-up and pain from weight-bearing.
Stopping the smoking will reduce the hyperhydrosis, thus allowing the majority of the punctate lesions to most likely resolve over a 2-3 months period of time. The main point is to control the hyperhydrosis to minimize the re-occurrence of these painful lesions.
Richard D Odom, DPM (Retired), Decatur, GA
01/18/2024
RESPONSES/COMMENTS (CLINICAL) - PART 1 A
From: Gary S Smith, DPM, Adrienne Sabin, DPM
I have had people improve greatly with Spenco insoles and spraying their feet daily with underarm antiperspirant spray.
Gary S Smith, DPM, Bradford, PA
Not knowing any other history of the patient, I suggest looking into Cowden’s syndrome as part of the differential diagnoses.
Adrienne Sabin, DPM, San Jose, CA
06/30/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1
RE: Low Tech Treatment for Heel Spur Deformity?
From: Richard Jaffe, DPM
On a trip to India, a common treatment for heel spur syndrome there was demonstrated to me by a local physician. A small, pointed hammer was heated and applied to the plantar heel, burning the skin.
 |
Low Tech Treatment for Heel Spur Deformity? |
The patient, who has had this treatment on two previous occasions told me that, in the past, it has helped her for about 2 years. Perhaps, if all else fails…
Richard Jaffe, DPM, Jerusalem, Israel
06/28/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1
From: Allen Jacobs, DPM
Generally, the medial malleolus does not begin to ossify until the seventh year. The differential diagnosis ranges from calcaneal valgus of infancy to occult tarsal coalition to any number of causes for chronic, progressive, collapsing foot deformity, such as ligamentous, laxity and associated disorders, compensating, deformities, and so forth.
Honestly, if you were asking such a question, it would be best that you refer the care of this patient for evaluation to those with more experience in the treatment of pediatric deformities of the foot.
Allen Jacobs, DPM, St. Louis, MO
06/22/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1C
From: David Secord, DPM
Every few years, the topic of prolotherapy seems to rear its head. The detractors point out that there are no studies establishing efficacy. Its supporters point out their level V (in the hierarchy of clinical evidence schema) success rates in their patient base. If anyone cares, here is some background:
From an interview with Dr. Paul H. Goodley, MD, by Carol Peckham Published: 08/19/2009:
Dr Goodley: Prolotherapy, [otherwise known as] regenerative injection therapy (RIT) or reconstructive ligament therapy, was developed about 60 years ago and is a fundamental, effective injection therapy for the repair of injured connective tissues, such as ligaments and tendons. Sclerotherapy and prolotherapy had previously been used...
Editor's note: Dr. Secord's extended-length letter can be read here.
06/22/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: Elliot Udell, DPM
Glen, thank you for enlightening us on your successes with prolotherapy. Perhaps you can publish your technique as well as findings. If you can document that prolotherapy works, the treatment will no longer be in the realm of alternative healthcare. If the article is well written, there are many journals in our profession that would love to publish it. As for charges, I based this on what a certain non-podiatric physician in my geographic area was charging and it was well over a thousand dollars for each treatment. Some of these patients were quite upset after spending 10K, out-of-pocket, for a series of dextrose injections.
Elliot Udell, DPM, Hicksville, NY
06/22/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1A
From: Robert Kornfeld, DPM
Dr. Ribotsky implores me to "publish my outcomes". But not having lived in my shoes, he does not understand. I will explain. There are 2 parts to the story. 1) I adopted a more holistic paradigm in 1987 after a chronic illness (which could not be helped by any conventional doctors for a few years) was healed and resolved within 3 months of seeing a holistic internist. I experienced the power of natural healing firsthand. I dove into learning everything I could and began experiencing its power on my patients.
I wanted to share this with the profession so I spent a number of years lecturing about the things I do to assist my patients to heal. Although I was invited to speak a number of times at large podiatric conventions, my efforts were not being well received by the podiatric community. So I started trying...
Editor's note: Dr. Kornfeld's extended-length letter can be read here.
05/24/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: David Secord, DPM
A few years back, I wrote a book on pain management, but never found a publisher. There was a chapter on the use of potentiation so that you could obtain greater effect from a narcotic and use a lower dosage via use of a potentiator drug. There are different categories (tricyclics, anti-psychotics, anxiolytics, SSRIs), but they work the same way (the explanation of which is too long to cover here.)
Navane (Thiothixene), Xanax (alprazolam), and a few others have been used to varying effect. When I did an office procedure in my surgical room, I would have the patient take a Vicoprofen (hydrocodone and ibuprofen) [now discontinued] with a 5mg or 10mg Valium (diazepam) (dosage dependent upon body mass) with food about an hour pre-op. The majority of the patients slept through the procedure and the ones who were conscious appeared completely at ease and relaxed. The one med would potentiate the effect of the other without increased mu receptor activation and respiratory depression.
David Secord, DPM, McAllen, TX
05/24/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1A
From: Steven Finer, DPM, Walter Perez, DPM
Try increasing the Ativan to 2.5mg. or consider 10mg. of Valium which has a longer life. Watch out for interactions with other drugs. Also, patients sometimes complain of headache after Valium. It also has mild muscle relaxant properties.
Steven Finer, DPM, Philadelphia, PA
I have not prescribed anti-anxiety medication for a long time for any type of surgery, including bone surgery, but if I have a very anxious patient, I prescribe Valium 5mg, two tablets, and ask the patient to take one tablet with a sip of water 2 hours before the surgery and if still anxious the second tablet 1 hour prior to the surgery. But what I really believe helps the patient's anxiety is to prepare them for surgery thoroughly, explain to them what to expect at the surgical center or hospital, step by step, and address their questions and concerns. That will help patients stay more relaxed and comfortable. My advice is to spend time with the patient going through the surgery and the process, and you may not need anxiolytics. I try to avoid them and I usually let the anesthesiologist handle anxiety issues.
Walter Perez, DPM, Brooklyn, NY
05/04/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1B
From: Wenjay Sung, DPM, Todd Lamster, DPM
That’s cancer. Prove me wrong; get a biopsy or send out for a biopsy.
Wenjay Sung, DPM, Arcadia CA
Regarding the unidentified lesion on the dorsal aspect of the foot, this lesion needs to be biopsied as soon as possible to rule out carcinoma. With its rolled border, I would guess that it is a basal cell carcinoma.
Todd Lamster, DPM, Scottsdale, AZ
05/04/2023
RESPONSES/COMMENTS (CLINICAL) - PART 1A
From: Thomas A. Graziano, DPM, MD, Alec Hochstein, DPM
There is not much history provided in the post regarding this "lesion" or even its duration. But in response to the poster question "any idea of what this might be?" I suggest a prudent approach would be first taking a biopsy of the lesion.
Thomas A. Graziano, DPM, MD, Clifton, NJ
In any seemingly healthy patient with a non-healing wound without specific etiology to point to for non-healing, a diagnosis of pyoderma gangrenous must be considered. Please keep us posted.
Alec Hochstein, DPM, Great Neck, NY
|
| |

|
|
|

